Tongue Tie in Babies: Symptoms, Diagnosis, Severity and What Parents Need to Know
Tongue tie (tethered oral tissues) is a common condition that can affect feeding, digestion and development in babies. This guide explains how to recognise the signs, understand severity, and know when to seek support. While tongue tie can play a role in feeding challenges, it’s often part of a bigger picture involving body tension, coordination and nervous system function.

Quick Links:
Tongue Tie in Babies: What Parents Need to Know
If feeding your baby feels harder than expected — painful, stressful, or just not quite right — you’re not alone.
Many parents are told:
“It’s normal”
“They’ll grow out of it”
Or “just give it time”
But when feeding continues to feel difficult, it’s often a sign that something isn’t functioning well.
One possible factor is tongue tie — but like most things in babies, it’s rarely the whole story.
This guide will help you understand what to look for, what matters, and what support can actually help.
What is Tongue Tie?
Tongue tie (ankyloglossia) refers to a restriction in the tissue under the tongue that may limit movement.
Some babies may also have:
Lip ties (upper lip restriction)
Buccal ties (cheek restrictions)
These can affect how the mouth functions during feeding — particularly the ability to:
Lift the tongue
Maintain suction
Coordinate sucking, swallowing and breathing
But here’s the key: Not all tongue ties cause problems — and not all feeding problems are caused by tongue tie.
Signs Your Baby May Have a Tongue Tie
Parents often notice that feeding just doesn’t feel right.
Common signs include:
Difficulty latching or staying latched
Clicking sounds during feeding
Painful breastfeeding or nipple damage
Long feeds that don’t seem satisfying
Reflux-like symptoms or excess wind
Dribbling milk or losing suction
Lip blisters
Preference for one side
These signs don’t confirm a tongue tie — but they do indicate that feeding isn’t working as smoothly as it should.
“If feeding feels hard, it’s worth understanding why — not just waiting it out.”
How is Tongue Tie Diagnosed?
Tongue tie is typically assessed by trained providers such as:
Lactation consultants (IBCLCs). -> In our opinion an IBCLC is the best practitioner to diagnose this
Dentists or oral health practitioners
Paediatric specialists
Assessment includes:
Visual examination of the tissue
Functional assessment (how the tongue moves)
Feeding observation
Diagnosis should never be based on appearance alone — function matters most.
Classes of Tongue Tie Severity
Tongue ties are often described in levels or classes, depending on how restrictive they are.
These range from:
Class 1: Mild, 12-16 millimeters
Class 2: Moderate, 8-11 millimeters
Class 3: Severe, 3-7 millimeters
Class 4: Complete, less than 3 millimeters
However: Severity doesn’t always match symptoms.
Things That Can Look Like Tongue Tie (But Aren’t)
Not all feeding challenges are caused by a tie.
Other contributing factors include:
Neck tension or birth strain
Jaw restriction
Cranial restriction/ cranial faults
Lumbo pelvic restriction
Nervous system dysregulation
Poor coordination of sucking/swallowing
Positioning or latch mechanics
This is why some babies:
Are told they have a tongue tie — but don’t improve after release
Or are told everything is “fine” — when feeding is clearly not working
Potential Impacts of Untreated Tongue Tie
When a tongue tie is functionally impacting feeding, it may contribute to:
Ongoing feeding difficulties
Digestive discomfort (wind, reflux-like symptoms)
Poor weight gain
Sleep disruption
Increased stress for both baby and parent
Early support can make a significant difference.
A More Complete View on Tongue Tie (Our Perspective)
Please not this next section isn’t to our knowledge well researched or documented - it’s our clinical experience and opinion
Tongue tie has become one of the most talked about — and misunderstood — topics in infant care.
On one hand, awareness has improved. More families are recognising feeding challenges earlier and seeking support.
On the other, it’s become a double-edged sword.
We’re seeing two patterns play out:
👉 Some babies are being labelled as having tongue tie when the real issue is tension, positioning or coordination
👉 While others — especially posterior tongue ties — are still being missed completely
The Double-Edged Sword
Not every feeding challenge is caused by a tongue tie.
Sometimes what looks like a restriction is actually:
Neck or jaw tension
Birth-related strain
Nervous system dysregulation
Poor coordination of sucking and swallowing
In these cases, addressing the body can significantly improve feeding — without the need for intervention.
But equally:
True tongue ties are still under-recognised — particularly posterior ties
These are often harder to see but can have a significant impact on:
Latch quality
Feeding efficiency
Long-term oral function
Why We Look Beyond Feeding Alone
One of the biggest misconceptions is that: “If feeding is okay, the tongue tie isn’t a problem.”
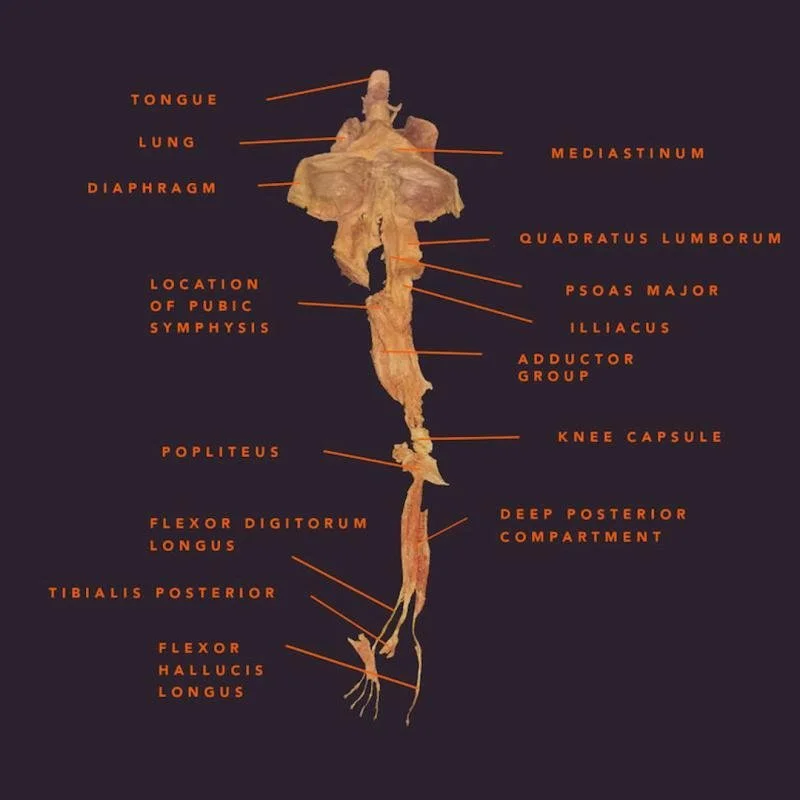
But the tongue is not an isolated structure.
It’s deeply connected through the fascial system — a continuous web of connective tissue — that links:
The tongue
The jaw
The diaphragm
The spine
And even down through the body
Keeping in mind the mouth is the start of digestion as well…. so it can impact the gut.
This means restriction in the tongue can influence more than just feeding.
Over time, this may contribute to patterns such as:
Mouth breathing
Altered facial, palate, teeth positioning and airway development
Tension through the jaw (TMJ) and neck
Changes in posture and movement patterns
There is also growing awareness of links between oral function, breathing patterns and:
Sleep quality
Nervous system regulation
Stress and anxiety responses
Immune response
Primitive Reflexes ( their effectiveness/activity and then integration)
While not every tongue tie leads to these outcomes, it highlights why function matters beyond the early feeding stage.
A comment on mouth breathing:
Mouth breathing is often less a standalone issue and more a sign that nasal breathing is not functioning well — commonly due to factors such as nasal obstruction, enlarged adenoids, rhinitis or sleep-disordered breathing. When this pattern persists, it can influence how a child breathes, sleeps and regulates their body. Research has shown associations between mouth breathing or sleep-disordered breathing and issues such as poor sleep quality, bedwetting (enuresis), recurrent ear and sinus problems, and air swallowing (aerophagia), which may contribute to digestive discomfort. There is also emerging discussion around how chronic mouth breathing may impact stress physiology and overall regulation through its effect on sleep and breathing patterns. While these relationships are not always direct or causative, they highlight the importance of understanding why a child is mouth breathing, rather than viewing it in isolation.¹²³⁴⁵
The Tongue, the Diaphragm and the Nervous System
The tongue and diaphragm are closely connected through both fascial and neurological pathways.
This relationship plays a role in:
Breathing patterns
Regulation of the nervous system
Feeding coordination
When these systems are not working together well, babies may present with:
Shallow or inefficient breathing
Increased tension or restlessness
Difficulty settling
Supporting the body — not just the tongue — can help improve how these systems work together.
“The goal isn’t just to ‘fix a tie’ — it’s to support how the whole system functions.”
Potential Long-Term Patterns We Consider
While every child develops differently, and not all tongue ties lead to issues, there is increasing clinical awareness that unresolved restriction may contribute to patterns seen later in life.
These may include:
Jaw & TMJ (TMD) Patterns
Jaw tension or clicking
Teeth grinding (bruxism)
Uneven bite development
TMJ discomfort or dysfunction
The tongue plays a key role in how the jaw develops and stabilises over time.
Dental & Oral Development
Crowding of teeth
Narrow palate or airway space
Mouth breathing patterns
Proper tongue positioning helps guide optimal oral and facial development.
Neck & Shoulder Tension
Ongoing neck tightness
Shoulder compensation patterns
Head-forward posture
Contributing to headaches
Restrictions in the tongue and jaw can influence how the upper body organises and moves.
Whole-Body & Movement Patterns
Because of the fascial connections through the body, some clinicians also observe links between oral restrictions and:
Postural imbalances
Movement inefficiencies
Compensatory patterns extending down the body
This may influence how force is distributed through the system — including the hips, knees and even feet over time.
Important Note
👉 These potential longer-term associations are based on clinical experience and emerging understanding of fascial and neurological connections.
They are not yet strongly established in long-term research, and not every child with a tongue tie will experience these outcomes.
It Takes a Team: Why Collaborative Care Matters
Tongue tie is rarely a one-provider solution.
The best outcomes often come from collaboration between:
Lactation consultants
Tongue tie practitioners
Bodyworkers (like chiropractors, physios or osteos)
👉 Each plays a role in supporting feeding, function and development.
How Chiropractic Fits In
While chiropractors don’t diagnose or release tongue ties, they can play an important role in supporting:
Tension through the neck and jaw
Nervous system regulation
Feeding coordination
Pre and post-release adaptation
👉 This is often the missing piece for babies who are still struggling.
Not Sure What’s Going On With Your Baby’s Feeding?
If you’re noticing signs of tongue tie or feeding challenges, the next step is understanding how it’s affecting your baby’s body — not just their mouth.
LEARN MORE: about our Tongue Tie Assessments in Mosman and how we support babies before and after release
The point of this…
As you can tell, there’s so much to consider when assessing and potentially addressing a tongue tie. Is it there? Is it not? Is it impacting feeding; is it causing mouth breathing and changing the facial structure? Or is it causing increased or asymmetrical body tension? Will it impact shoulder mobility, ability to open their mouth, or neck range of motion… and impact ability to do tummy time or learn to roll both directions? Is it impacting their vagus nerve, their sense of safety and calm; and impacting sleep and feeding? Is it impacting the primitive reflexes associated with sucking, rooting, feeding? That’s where we come in…
It’s not something we casually address. It’s complex. And it’s a big decision to have it revised.
In our experience, if you’re going to do the revision, it’s a smoother process when done sooner rather than later.. in part because the tissue is still very thin and elastic and easier to either laser or cut (practitioner dependent - and note we are not the practitioners doing the revisions, we co-manage with the Doctors and Dentists who perform the procedure.)
We can’t tell you what to do, nor can we predict the future of what it might (or might not!) cause. All we can do is tell you what we do know… and help you to fact find. And with as much clinical information as you can digest, make your own educated decision on what’s best for you, your baby, your family.
Our part → we will help to resolve any underlying joint restrictions that could be contributing to their range of motion, structure/function and nervous system regulation. And assist in the pre and post work when and if revision is the decision you make.
We have your team (IBCLC, Dentist etc) on speed dial. We will collaborate on what we are all finding and try and help you to make your decision. And support you with whatever it is that you decide. Whether you choose to use our recommended providers or come to us with your ready chosen team. We’ve got your back
Providers we work with frequently work with:
Dentists:
Dr Louis Chan (My Dental Care - Meadowbank)
Dr Suttner Haddad (Bondi Dental)
Dr Jason Pang (Cosmic Smile Laser Dental - Neutral Bay)
Speech Pathologists:
Cordelia Van Aalst (Sydney Speech Team)
Lactation Consultants (IBCLC):
North Shore & Northern Beaches:
Felicity Hughes (Motherhood Matters)
Elle Lee (Motherhood Matters)
Leonie Clements (Motherhood Matters)
Hills District
Trish Doyle - Nurturing Well
Central Coast
Harriet Blannin-Ferguson (The Breast Help)
Tongue Tie Frequently Asked Questions
1) How do I know if my baby has a tongue tie?
There isn’t one single sign that confirms a tongue tie, but there are common patterns parents notice. These include difficulty latching, clicking sounds during feeding, painful breastfeeding, long feeds that don’t seem satisfying, reflux-like symptoms, or an unsettled baby.
It’s important to understand that these signs don’t automatically mean a tongue tie is present — they simply indicate that feeding isn’t functioning well. A proper assessment looks at both the structure of the tongue and how it moves during feeding.
2) What are the most common symptoms of tongue tie in babies?
The most common symptoms are related to feeding. Babies may struggle to latch effectively, lose suction during feeds, or appear frustrated or fatigued while feeding. Parents may experience nipple pain or damage, especially during breastfeeding.
Other signs can include excessive wind, reflux-like symptoms, dribbling milk, or a baby who feeds frequently but still seems unsettled. Some babies also show tension through the neck or prefer turning their head to one side.
3) Can a baby have a tongue tie and still feed normally?
Yes — not all tongue ties cause problems. Some babies have a visible tie but feed well and show no signs of difficulty. In these cases, no treatment may be needed.
What matters most is function, not just appearance. A baby with a mild-looking tie may struggle significantly, while another with a more obvious restriction may have no feeding issues at all. This is why assessment should always focus on how the baby is feeding and functioning.
4) How is tongue tie diagnosed?
Tongue tie is usually assessed by trained providers such as lactation consultants (IBCLCs), dentists, or paediatric practitioners. The assessment includes both a visual check of the tissue and a functional assessment of how the tongue moves.
Feeding observation is a key part of the process. This helps determine whether the tongue restriction is actually impacting latch, suction, and coordination. Diagnosis should never be based on appearance alone — function is the most important factor.
5) Should all tongue ties be treated or released?
No — treatment decisions should be based on whether the tongue tie is affecting function, particularly feeding. If a baby is feeding well and developing normally, a release may not be necessary. But also remember it’s your baby, your gut instinct, your choice.
If feeding is difficult, painful, or not improving with support, a release may be considered as part of a broader care plan. This decision is best made with guidance from experienced providers who understand both feeding and oral function.
And also that some babies present with a tongue tie, but if there is neuromusculoskeltal restriction/fixation it can make it appear to be a tie…. so bodywork is imperative to ensure you’re heading down the right track.
6) Why doesn’t feeding always improve after a tongue tie release?
A tongue tie release changes the structure, but feeding is a learned and coordinated process involving the whole body. If a baby has developed compensations or tension patterns, these don’t automatically resolve after the procedure.
This is why some babies continue to struggle after a release. Supporting the body, improving coordination, and allowing time for integration are often key parts of improving feeding outcomes.
7) What else can cause feeding problems if it’s not a tongue tie?
Feeding challenges can also be influenced by factors such as neck tension, jaw restriction, birth-related strain, nervous system regulation, or difficulties coordinating sucking and swallowing.
In many cases, it’s not just one issue but a combination of factors. This is why a whole-body assessment can be helpful in understanding what’s contributing to feeding difficulties.
8) When should I get my baby checked for feeding issues?
If feeding feels painful, stressful, or not improving, it’s worth having your baby assessed. Early signs like poor latch, unsettled behaviour, or reflux-like symptoms can indicate that something isn’t functioning well.
Many parents are advised to “wait and see,” but early support often leads to better outcomes and a more positive feeding experience for both baby and parent.
9) Who should I see if I think my baby has a tongue tie?
A lactation consultant (IBCLC) is often the best first step, as they can assess feeding and provide guidance. Depending on what’s found, they may refer to a dentist or other practitioner for further assessment.
A team-based approach is often most effective, especially when feeding challenges are ongoing or complex.
-
⚠️ Disclaimer:
This information is educational only and is not intended to replace individual medical advice. Chiropractors do not claim to “treat” medical conditions in infants. If you have concerns about your baby’s health or development, please consult your GP, paediatrician, or other qualified health professional. -
Australian Breastfeeding Association
Tongue-tie and breastfeeding
https://www.breastfeeding.asn.au/resources/tongue-tieLa Leche League International
Tongue and Lip Ties
https://www.llli.org/breastfeeding-info/tongue-lip-ties/International Lactation Consultant Association
Clinical guidelines and resources on infant feeding and oral function
https://ilca.orgnternational Chiropractic Pediatric Association
Tethered Oral Ties and Chiropractic Care
https://icpa4kids.comAmerican Academy of Pediatrics
Identification and Management of Ankyloglossia
https://publications.aap.orgNational Institutes of Health
Ankyloglossia (Tongue-Tie) and Breastfeeding Outcomes
https://www.ncbi.nlm.nih.govCochrane Library
Frenotomy for tongue-tie in newborn infants
https://www.cochranelibrary.comAcademy of Breastfeeding Medicine
Clinical Protocol #11: Guidelines for the evaluation and management of neonatal ankyloglossia
https://www.bfmed.orgAustralian Spinal Research Foundation
Neurological development and infant care resources
https://spinalresearch.com.auAustralian Chiropractic Association
Chiropractic care and paediatric populations
https://www.chiro.org.auHeidi Haavik
The Reality Check: A Quest to Understand Chiropractic from the Inside Out
https://realitycheckbook.comNational Institutes of Health
Sleep-Disordered Breathing and Paediatric Outcomes
https://www.ncbi.nlm.nih.govCleveland Clinic
Aerophagia (Air Swallowing)
https://my.clevelandclinic.org/health/diseases/aerophagiaAmerican Academy of Pediatrics
Obstructive Sleep Apnea in Children
https://publications.aap.orgNational Institute of Diabetes and Digestive and Kidney Diseases
Bedwetting (Enuresis) and Sleep
https://www.niddk.nih.govNational Library of Medicine
Mouth Breathing and Upper Airway Function
https://pubmed.ncbi.nlm.nih.gov
Want to learn more? Book a FREE 15min discovery call with one of our Sydney Baby & Tongue Tie Chiropractors today: Book HERE
Tongue tie can impact feeding, comfort and development, but it’s not always the sole cause of feeding challenges. Understanding symptoms, function and contributing factors is key. A collaborative approach — including feeding support and body-based care — often leads to the best outcomes for babies and families.